肺炎¶
up:: 專師考試解題
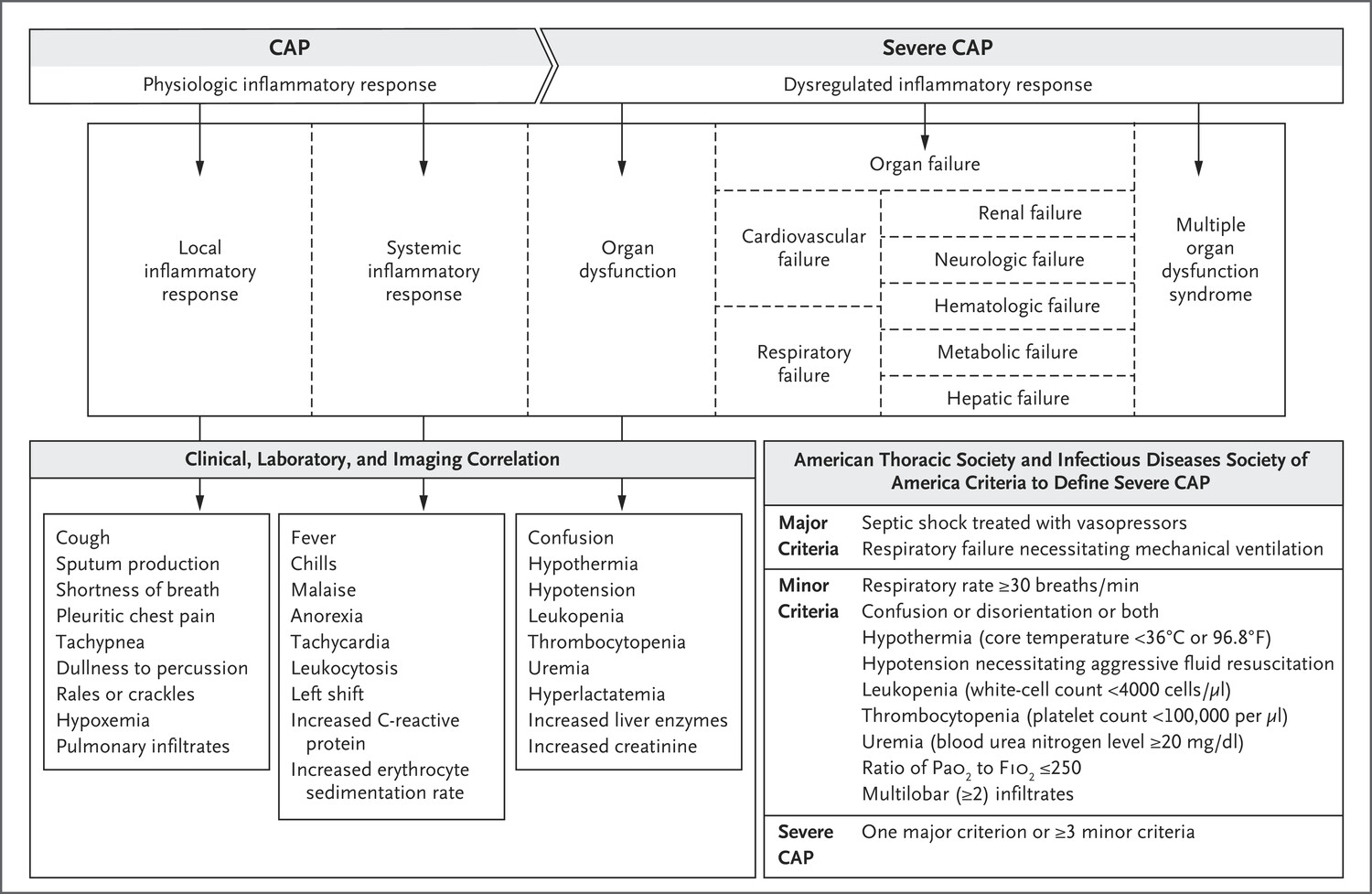
Definitions and clinical manifestations¶
- Pneumonia: s/s (fever, cough, purulent sputum, dyspnea) + new infiltrate on chest imaging
- Community-acquired pneumonia (CAP): pneumonia acquired outside of hospital setting
- Hospital-acquired pneumonia (HAP): pneumonia acquired ≥48 hrs after hospitalization
- Ventilator-associated pneumonia (VAP): pneumonia acquired ≥48 hrs after intubation
- Lung empyema: accumulation of pus in pleural space
- Lung abscess: parenchymal necrosis with confined cavitation
- Aspiration pneumonitis: acute lung injury after inhalation of gastric contents without infection, though bacterial infection can occur within 24–72 hrs of injury
Microbiology of Pneumonia¶
| Clinical Setting | Etiologies |
|---|---|
| CAP (AJRCC 2019;200:7) | No pathogen identified in 50–60%, virus alone in ~25%, bacteria alone in ~10%, virus-bacteria coinfection in <5% Viruses: influenza, RSV, hMPV, parainfluenza, rhinovirus, coronavirus S. pneumoniae (most common bacterial cause) S. aureus (espec. post-influenza) Mycoplasma, Chlamydia (espec. in young & healthy) H. influenzae, M. catarrhalis (espec. in COPD) Legionella (espec. in elderly, smokers, ↓ immunity, TNF inhibitors) Klebsiella & other GNR (espec. in alcoholics & aspiration) |
| HAP/VAP | S. aureus, Pseudomonas, Klebsiella, E. coli, Enterobacter, Acinetobacter, Steno. IV abx w/in 90 d risk factor for MDR. Viral ~20% cases. |
| Empyema | S. pneumo, S. aureus, E. coli, Klebsiella, H. influenzae, anaerobes |
| Lung abscess | Often polymicrobial, incl. oral flora. S. aureus, anaerobes, Strep (anginosus, GAS), GNR (Klebsiella, E. coli, Pseudomonas), Nocardia, Actinomyces, fungi, mycobacteria, Echinococcus |
| Immunosupp. | Above + Pneumocystis, Cryptococcus, Nocardia, non-TB myco- bacteria (NTM), CMV, invasive molds |
| Pathogen Group | Pathogen |
|---|---|
| Common or core | |
| Gram-positive bacteria | Streptococcus pneumoniae, methicillin-susceptible Staphylococcus aureus, Strep. pyogenes, other streptococci |
| Gram-negative bacteria | Hemophilus influenzae, Moraxella catarrhalis, Enterobacteriaceae (e.g., Klebsiella pneumoniae) |
| Atypical bacteria | Legionella pneumophila, Mycoplasma pneumoniae, Chlamydophila pneumoniae |
| Respiratory viruses | Influenza virus, SARS-CoV-2, respiratory syncytial virus, parainfluenza virus, human metapneumovirus, rhinoviruses, common human coronaviruses |
| Uncommon or infrequent | |
| Gram-positive bacteria | Methicillin-resistant Staph. aureus, nocardia species, Rhodococcus equi |
| Gram-negative bacteria | Enterobacteriaceae, including extended-spectrum beta-lactamases or carbapenem-resistant enterobacteriaceae; nonfermenting bacilli (e.g., pseudomonas or acinetobacter); Francisella tularensis |
| Atypical bacteria | Chlamydia psittaci, Coxiella burnetii |
| Mycobacteria | Mycobacterium tuberculosis, nontuberculous mycobacteria |
| Viruses | Cytomegalovirus, herpes simplex, varicella zoster, MERS-CoV |
| Fungi | Pneumocystis jirovecii, aspergillus species, mucorales species, histoplasma species, cryptococcus species, blastomyces species, coccidioides species |
| Parasites | Strongyloides stercoralis, Toxoplasma gondii |
| CAP Pathogen | Specific Risk factors |
|---|---|
| Influenza | Influenza activity in the community. Close contact with an infected person. |
| SARS-CoV-2 | SARS-CoV-2 activity in the community. Close contact with an infected person. |
| Legionella species | Recent cruise ship. Exposure to contaminated water sources (e.g., hot tubs, cooling towers; recent plumbing) |
| MRSA | Prior infection or colonization with MRSA |
| Pseudomonas aeruginosa | Prior infection or colonization withPseudomonas aeruginosa |
| MDR Gram-negative rods | Prior infection or colonization with MDR Gram-negative rods |
| Oral anaerobic bacteria | Poor dental hygiene |
| Chlamydophila psittaci | Exposure to birds |
| Coxiella burnetti | Exposure to farm animals or parturient cats |
| Francisella tularensis | Exposure to rabbits |
| MERS-CoV | Exposure to infected camels; travel to the Arabian Peninsula |
| Coccidioides species | Travel to southwestern United States |
| Histoplasma capsulatum | Exposure to bat or bird droppings |
Diagnostic studies¶
(AJRCC 2019;200:e45)
- Sputum Gram stain/Cx:
- Reliable if high quality (ie, sputum not saliva; <10 squam cells/lpf).
- If bacterial PNA should be purulent (>25 PMN/lpf).
- Yield ↓ >10 h after abx (CID 2014;58:1782).
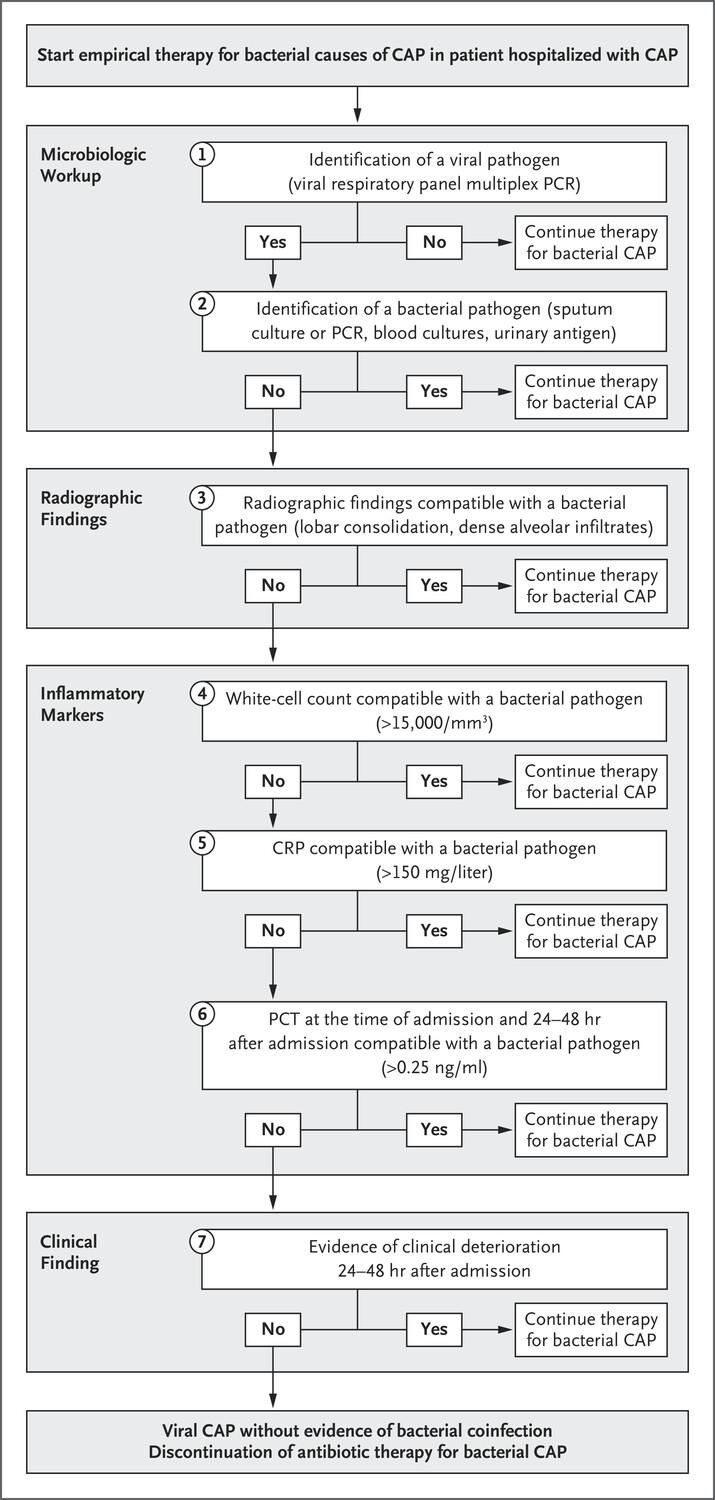
- Procalcitonin: ↑ in acute bacterial (not viral) PNA.
- Consider stopping abx if levels <0.25 ng/ml (<0.5 ng/mL in ICU Pts) or ↓ ≥80% from peak. ↓ abx exposure by 2–3 d (Lancet ID 2016;16:819 & 2018;18:95).
- Not validated in immunosuppressed hosts.
- Levels harder to interpret in CKD.
- False ⊕ in cardiac arrest, shock, burns, surgery.
- CXR (PA & lateral)
- HIV test (if unknown)
- MRSA nares swab in HAP/VAP (if ⊖ 96% NPV for MRSA PNA)
- Consider in severe disease (otherwise not recommended):
- Legionella urinary Ag (detects L. pneumophila L1 serotype, 60–70% of clinical disease)
- S. pneumoniae urinary Ag (Se 70%, Sp >90%)
- Blood cultures (before antibiotics!): ⊕ in ~10% of inPts, depending on pathogen
- If clinical suspicion for mTB:
- (induced) sputum AFB stain ×3 q ≥8h (w/ ≥1 early morning).
- Mycobact. cx (empiric respiratory isolation while pending)
- MTb DNA PCR if smear ⊕
- Viral testing (DFA or PCR) on nasopharyngeal swab or sputum
- Bronchoscopy: immunosupp., critically ill, failure to respond, suspected PCP, inadequate/ ⊖ sputum cx
- Send Gram stain/cx, Legionella cx, fungal cx/wet prep, mycobacterial cx/smear, modified AFB stain, galactomannan
- Reasons for failure to improve on initial treatment:
- Insufficient time: may take ≥72 h to see improvement (fever persists >4 d in ~20%)
- Insufficient drug levels for lung penetration (eg, vanco trough <15–20 μg/mL)
- Resistant organisms or superinfxn: eg, MRSA, Pseudo.; consider bronchoscopy
- Wrong dx: fungal/viral, chemical pneumonitis, PE, CHF, ARDS, DAH, ILD; consider CT
- Parapneumonic effusion/empyema/abscess: if CXR ⊖, consider bedside US or CT. If effusion >1 cm, drain & send fluid pH, gluc, Gram stain & Cx.
- Metastatic infection (eg, endocarditis, septic arthritis)
Triage¶
- qSOFA predicts poor outcomes, prolonged ICU stay, and in-hospital mortality if >2 of 3: RR>22, AMS, SBP<100 (JAMA 2016; 315:801)
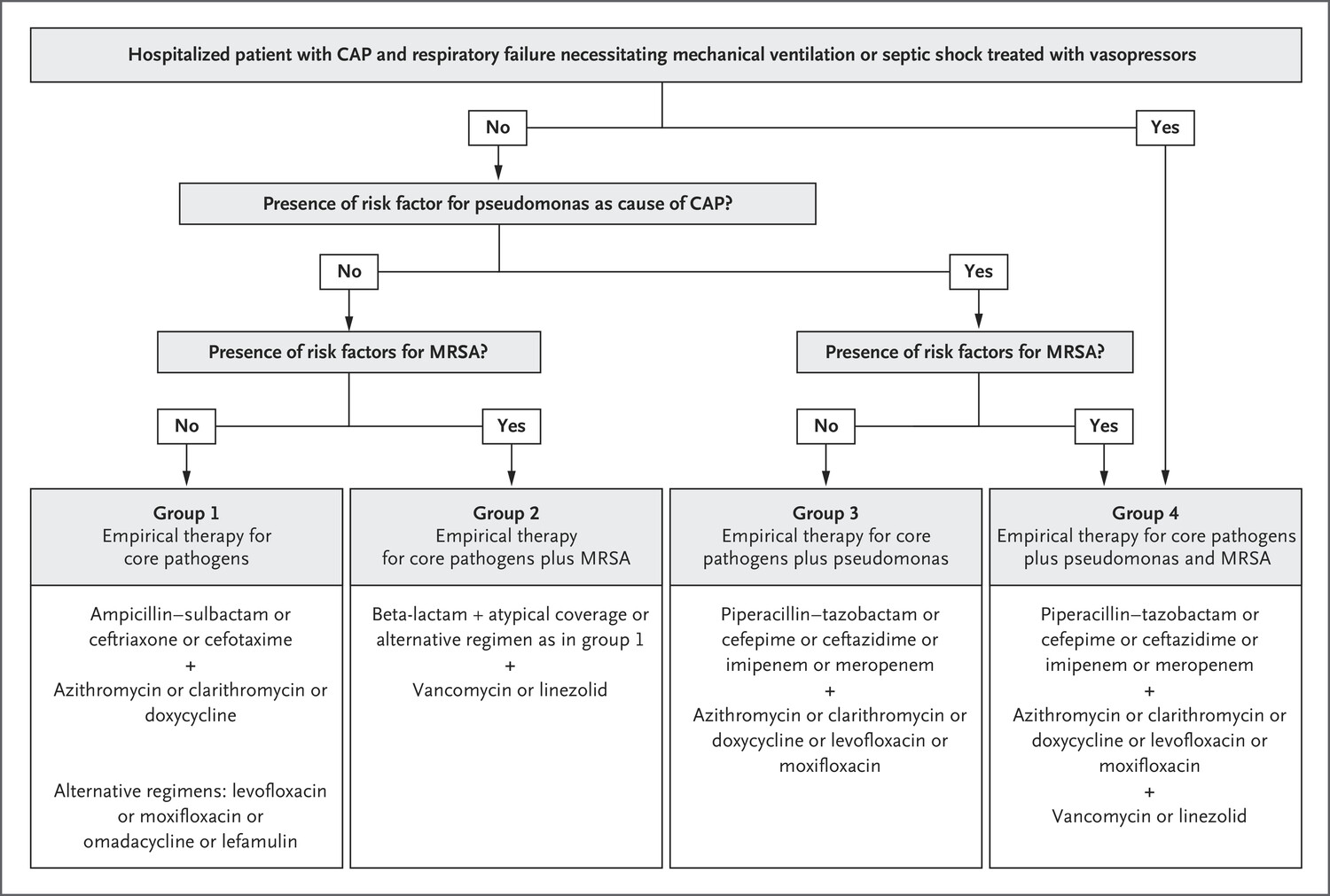
Treatment¶
(NEJM 2019;380:651; AJRCC 2019;200:e45)
- Avoid quinolones if suspect TB. When possible, de-escalate abx based on sensitivities.
- Steroids: not unless indicated for shock or COPD exacerbation; may ↓ mortality, mech vent, & ARDS in severe CAP (Cochrane 2017;12:CD007720). Avoid in influenza.
- Duration:
- CAP: 5–7 days, can de-escalate IV abx to PO after clinical improvement.
- HAP/VAP: 7 days.
- Empyema/abscess: 2–6 wks based on complexity, drainage.
| Scenario | Regimen |
|---|---|
| CAP (outPt) | Amoxicillin, azithro, or doxy (avoid latter two if >25% resistance locally) |
| CAP (ward) | [3rd-gen ceph + azithro] or levoflox; omadacycline ≍ FQ (NEJM 2019;380:517) |
| CAP (ICU) | 3rd-gen ceph + azithro. Only cover MRSA or Pseudomonas if risk factors (prior PsA PNA, MRSA infection, recent hospitalization, IV abx) |
| HAP/VAP | [Pip-tazo or cefepime or carbapen.] + [vanc or linezolid]. May add resp FQ or azithro if concerned for atypicals. Daptomycin not active in lungs. |
| Empyema/ abscess | [3rd-gen ceph + MNZ] or amp-sulbactam. Only cover Pseudomonas or MRSA if risk factors. Empyema: drain if >1 cm ± chest tube. Abscess: drainage not required. De-escalate to PO abx based on clinical improvement & micro. |
Prevention¶
- All persons >65 or age 19–64 w/ CHF, lung disease, cirrhosis, DM, EtOH, smoker, immunosupp. (eg, ESRD, organ transplant, HIV, leukemia, lymphoma, asplenia)
- PCV20 vaccine or PCV15 + PPSV23 1 yr later
Viral Respiratory Infections¶
Presentation: URI, bronchitis, bronchiolitis, pneumonia (Lancet 2011;377:1264)
Microbiology & epidemiology¶
(http://www.cdc.gov/flu/weekly)
- Typical pathogens: Short, mild = rhinovirus, other non-SARS-CoV-2 coronavirus.
- Longer, more severe or complicated = influenza, parainfluenza, RSV, adenovirus, metapneumovirus, COVID-19 (vide infra). Can be esp. severe in immunosupp.
Diagnosis¶
- Sx: fever, cough, myalgias, SOB, wheezing, sore throat, rhinorrhea, malaise, confusion
- Respiratory viral panel on nasal swab or sputum/BAL; rapid flu nasopharyngeal swab preferred to nasal swab (Se 50–70%, Sp >90%); RT-PCR for flu A/B (>95% Se & Sp)
Treatment¶
(NEJM 2017;390:697)
- Influenza (A & B):
- Neuraminidase inhib. (eg, oseltamivir); must start w/in 48 h of sx for low-risk; for critically ill or immunosupp., start ASAP even if >48 h. Peramivir IV if unable to tolerate PO.
- Endonuclease inhib. (baloxavir): superior to oseltamivir in ↓ sx & viral load on 1st day of Rx, but resistance emerging; no data in severe influenza (NEJM 2018; 379:913)
- RSV: can consider inhaled ribavirin in immunosupp, but very expensive & rarely used
Prevention¶
- Inactivated influenza vaccine: rec for all >6 mo of age.
- Isolation, droplet precautions for inpatients strongly recommended
- Ppx for high-risk contacts of confirmed influenza: oseltamivir × 7 d or baloxavir single dose
考古題¶
專師¶
// Specify the path to the original note
const originalNotePath = "Area/Medicine/專師考試解題.md"; // Replace with your actual file path
// Read the content of the original file asynchronously
const content = await app.vault.read(app.vault.getAbstractFileByPath(originalNotePath));
// Define the tag you're searching for
const tag = "#medicine/pneumonia"; // Replace with your actual tag
// Split the content into sections based on the start of a new question (line with a number and a period)
const sections = content.split(/(?=\d+\.\s)/);
// Initialize an array to store the results
const results = [];
// Process each section
sections.forEach(section => {
if (section.includes(tag)) {
// Add the section to results if it contains the tag
results.push(section.trim());
}
});
// Output the captured sections
results.forEach(result => dv.paragraph(result));
內科醫師¶
// Specify the path to the original note
const originalNotePath = "Area/Medicine/內專考古題.md"; // Replace with your actual file path
// Read the content of the original file asynchronously
const content = await app.vault.read(app.vault.getAbstractFileByPath(originalNotePath));
// Define the tag you're searching for
const tag = "#medicine/pneumonia"; // Replace with your actual tag
// Split the content into sections based on the start of a new question (line with a number and a period)
const sections = content.split(/(?=\d+\.\s)/);
// Initialize an array to store the results
const results = [];
// Process each section
sections.forEach(section => {
if (section.includes(tag)) {
// Add the section to results if it contains the tag
results.push(section.trim());
}
});
// Output the captured sections
results.forEach(result => dv.paragraph(result));