HIV/AIDS
Source: Pocket Medicine, 2022
up:: 專師考試解題
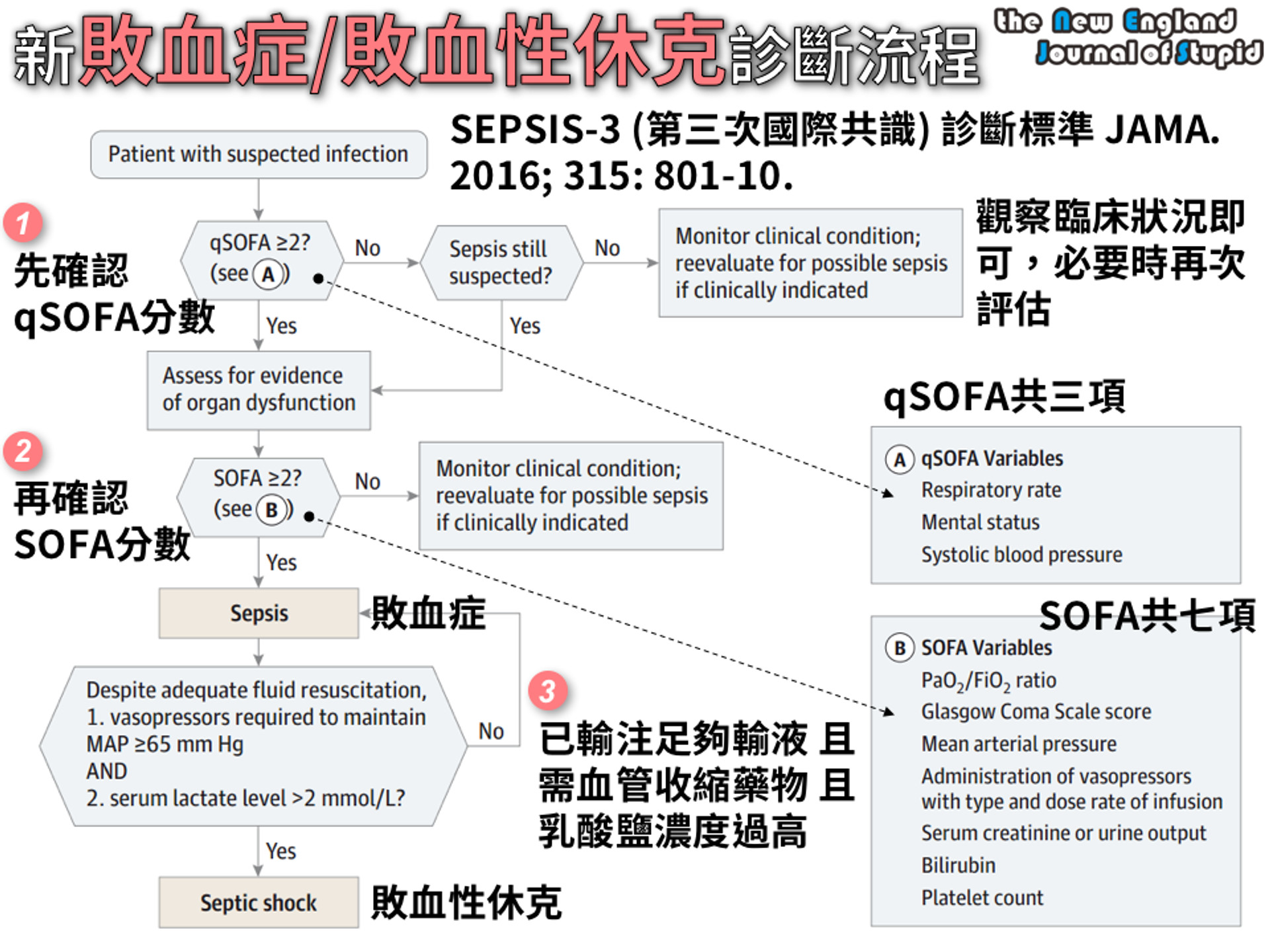
定義與臨床表現
- 急性HIV:皮疹、淋巴結腫大、發燒、口腔潰瘍、咽喉炎、肌肉疼痛、腹瀉
- 一般在接觸後約2-6週出現;並非所有HIV感染者會出現急性HIV的症狀
- 愛滋病(AIDS):HIV + CD4 <200/mm³ 或出現AIDS定義的伺機性感染(OI)或惡性腫瘤
HIV 感染中定義愛滋病(AIDS)的伺機性感染與指標性疾病
- HIV 引起的腦病變(Encephalopathy attributed to HIV)
- 進行性多灶性白質腦病變(Progressive multifocal leukoencephalopathy)
- 多次或反覆性細菌感染(僅限 6 歲以下兒童)
- 沙門氏菌敗血症,反覆發作
- 肺炎,反覆發作(僅限成年人、青少年及年滿 6 歲以上兒童)
- 支氣管、氣管或肺部念珠菌感染
- 食道念珠菌感染
- 播散性或肺外球孢子菌病(Coccidioidomycosis)
- 肺外隱球菌病(Cryptococcosis)
- 播散性或肺外組織胞漿菌病(Histoplasmosis)
- Pneumocystis jirovecii(舊稱 P. carinii)肺炎
- 巨細胞病毒感染(不含肝、脾或淋巴結),發病年齡 >1 個月
- 巨細胞病毒視網膜炎(合併視力喪失)
- 單純皰疹病毒感染:慢性潰瘍(持續 >1 個月)或支氣管炎、肺炎、食道炎(發病年齡 >1 個月)
- 播散性或肺外 Mycobacterium avium complex 或 Mycobacterium kansasii 感染
- 任一部位之結核病(Mycobacterium tuberculosis):肺結核(僅限成年人、青少年與年滿 6 歲以上兒童)、播散性或肺外結核
- 播散性或肺外感染的其他分枝桿菌或未鑑定分枝桿菌
- 侵犯性子宮頸癌(僅限成年人、青少年與年滿 6 歲以上兒童)
- 卡波西肉瘤(Kaposi sarcoma)
- 伯基特淋巴瘤(Burkitt lymphoma 或同等類型)
- 免疫母細胞淋巴瘤(Immunoblastic lymphoma 或同等類型)
- 原發性中樞神經系統淋巴瘤 (Primary CNS lymphoma)
- HIV 引起的惡病質症候群(Wasting syndrome attributed to HIV)
- 慢性腸道隱孢子蟲病(Cryptosporidiosis)(持續 >1 個月)
- 慢性腸道等孢子蟲病(Isosporiasis)(持續 >1 個月)
- 腦部弓形蟲病(Toxoplasmosis of brain),發病年齡 >1 個月
流行病學
- 約有120萬美國人與HIV感染共存(13% 不知道自己感染);全球約3700萬
- 高風險群體:男性同性戀者、變性女性、靜脈注射毒品者、性工作者、高風險患者的伴侶
- 傳播途徑:性行為(無抗病毒藥物時風險為0.1-1%)、針扎(職業或靜脈注射毒品)、垂直傳播(無抗病毒藥物時風險為15-40%)、輸血、器官移植(在美國不常見)
預防 (NEJM 2015;373:2237; Lancet 2016;387:53; J Infect Dis 2018;218:16; CDC 2021)
- 暴露前預防(PrEP):每日服用TDF/FTC,若遵守療程可減少超過90%的傳播風險。考慮用於HIV陰性伴侶、無安全套性行為的高風險群體、6個月內有性傳播感染史、靜脈注射毒品且共用針頭者。開始之前需排除HIV,並每3個月檢查腎功能、性病及HIV。
- 暴露後預防(PEP):在高風險暴露後盡快(72小時內)開始(如果HIV狀態不明則需要個別決定)。檢查基礎HIV、性病、HBV、HCV。治療:2種NRTI(通常是TDF/FTC)+ RAL或DTG × 4週。考慮後續開始PrEP。
篩檢與診斷 (JAMA 2018;320:379)
- 所有13-64歲人群至少篩檢一次,每次懷孕時、若有新性病感染診斷時篩檢;高風險者每年篩檢
- HIV抗體/p24抗原(ELISA檢測):感染後1-12週陽性;靈敏度超過99%;為主要篩檢測試
- 如果結果為陽性,抗體分型檢測可確認並區分HIV-1與HIV-2(MMWR 2013;62:489)
- 血漿HIV RNA PCR病毒量(VL):檢測範圍為20-1000萬拷貝/mL;偽陽性可能發生,但通常拷貝數量較少;相比之下,初期感染病毒量應該較高(>75萬)
- CD4計數:不是診斷測試,因為可能HIV陽性但CD4正常,或HIV陰性但CD4低
對新診斷HIV陽性患者的處理 (CID 2020;73:e3572)
- 諮詢關於若服藥遵從性高則治療預後良好、治療選擇及病情披露
- 實驗室評估:CD4計數、HIV病毒量及基因型、CBC/DC、基礎生化、肝功能、HbA1c、血脂肪、尿液分析、PPD/IGRA、梅毒抗體、披衣菌與淋病(3部位)、A/B/C型肝炎、G6PD(如果是高風險族群)、懷孕篩檢、若使用abacavir則檢查HLA-B*5701
- 如果是AIDS:CMV IgG、Toxo IgG。
- 確認所有疫苗(包括每年流感疫苗)都是最新的,若CD4 ≤200則避免使用活菌疫苗
- 及早開始抗病毒藥物(最好在實驗室檢查和基因型結果後,同時得到HIV專家指導),不論CD4數值如何,因為可以降低死亡率(NEJM 2015;373:795)
- 治療可以預防對伴侶的傳播。當病毒量檢測不到超過6個月時,無保護性行為的傳播風險約為0%(JAMA 2016;316:171;Lancet HIV 2018;5:e438)。
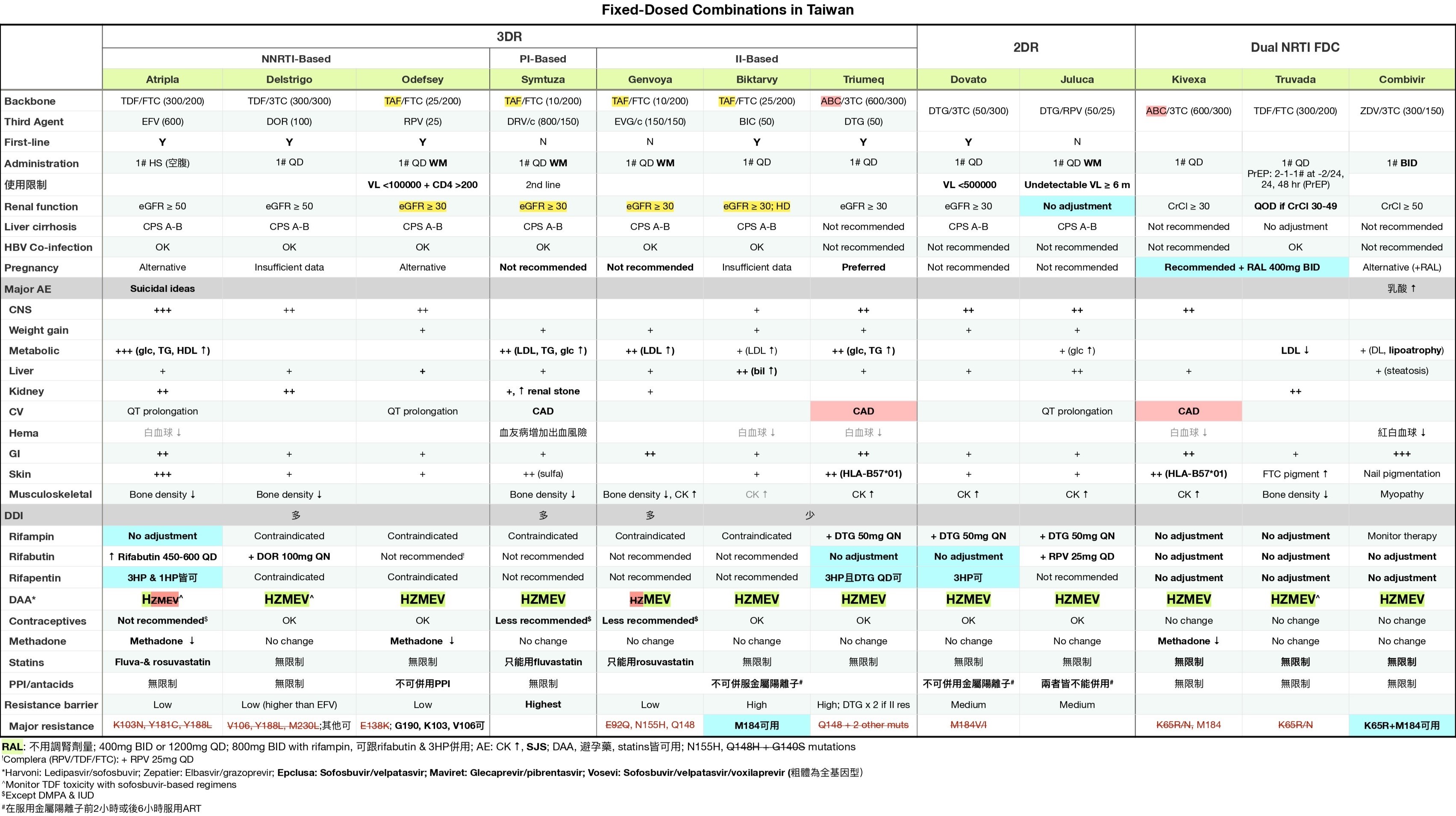
- 治療方案包括:2種NRTI(如TAF + FTC)+ INSTI或加強型PI(如DRV/r)
- 開始抗病毒治療可能會因免疫重建發炎症候群(IRIS)暫時加重現有的伺機性感染(TB、MAC、CMV等)。在抗病毒治療的前4週使用類固醇可降低TB相關IRIS的風險,但不建議常規使用(NEJM 2018;379:1915)。
- 如果擔心有隱球菌或TB腦膜炎,不應立即開始抗病毒治療
- 開始抗病毒治療後,需每4週檢查一次病毒直到達到不可檢測,之後每3-4個月監測一次
對之前已知HIV陽性患者的處理
- 病史與體檢(黏膜皮膚、神經認知、伺機性感染、惡性腫瘤、性病);藥物及依從性
- 回顧抗病毒藥物(過去和現在);如果住院,通常繼續使用抗病毒藥物,如果必須停用,則全部停止以降低抗藥性風險
- 治療失敗:在使用抗病毒藥物幾個月後無法達到不可檢測VL、病毒反彈(在之前的抑制後VL >200拷貝/mL ×2次)、CD4計數下降或臨床惡化
機會性感染預防
| 感染 | 指徵 | 初級預防 |
|---|---|---|
| 結核 | PPD陽性(≥5 mm)、IGRA或高風險暴露 | 參見潛伏結核的治療 |
| 肺囊蟲肺炎_Pneumocystis jiroveci_ (PCP) | CD4 <200/mm 或 CD4 <14% 或 口腔念珠菌感染 | TMP-SMX(首選)或dapsone或atovaquone或吸入pentamidine |
| 隱球菌 | CD4 <150/mm 且有地方流行/暴露史 | Itraconazole |
| 弓形蟲 | CD4 <100/mm³ 且Toxo IgG陽性 | TMP-SMX或dapsone 50 mg + pyrimethamine + leucovorin |
| MAC | 若已開始有效抗病毒藥物則不再建議預防 | |
| 停止預防的時間:若CD4 >200 × 3個月則停止PCP和弓形蟲的預防 |
HIV/AIDS的併發症
| CD4 計數 | 併發症 |
|---|---|
| 任何 | S. pneumonia、TB、VZV、HPV併發症、卡波西氏肉瘤、淋巴瘤、心血管疾病風險增加、骨密度降低 |
| <500 | 全身症狀。黏膜皮膚:脂漏性皮膚炎;牛皮癬;口腔毛狀白斑;HSV。反覆的細菌感染 |
| <200 | 肺囊蟲肺炎、弓形蟲、進行性多灶性白質腦病(PML)、隱球菌、念珠菌、球黴菌、組織胞漿菌 |
| <50-100 | 巨細胞病毒(CMV)、鳥型結核菌(MAC)、中樞神經系統淋巴瘤、侵襲性麴菌病、桿菌血管瘤(播散性_Bartonella_感染)、死亡(<50 是醫療急症) |
HIV/AIDS患者的發燒檢查
病因 (Infect Dis Clin North Am 2007;21:1013)
- 感染 (82-90%):鳥型結核菌(MAC)、TB、巨細胞病毒(CMV)、早期 肺囊蟲肺炎(PCP)、組織胞漿菌(Histoplasmosis)、隱球菌(Cryptococcosis)、球黴菌(Coccidioidomycosis)、弓形蟲(Toxoplasmosis)、心內膜炎
- 非感染性:淋巴瘤、藥物反應
- 非急性HIV感染本身很少 (<5%) 是發燒的主要原因
檢查:根據 CD4 計數、症狀、流行病學及暴露情況進行
- CBC、基礎生化、肝功能檢查、血液培養、胸部 X 光、尿液分析、分枝桿菌及真菌培養、檢查藥物、必要時檢查胸部及腹部 CT
- CD4 <100-200 → 血清隱球菌抗原、尿液組織胞漿菌抗原、CMV PCR
- 呼吸系統症狀 → 胸部 X 光;動脈血氧分析;痰液細菌培養、PJ染色、抗酸桿菌檢查;支氣管鏡檢查
- 腹瀉 → 糞便培養、卵蟲檢查、抗酸桿菌檢查;如有必要,進行結腸鏡檢查以直接觀察和取樣
- 血液學異常 → 骨髓切片以進行病理檢查及培養,包括分枝桿菌及真菌的檢查
- 頭痛/視力變化 → 腰椎穿刺;將腦脊髓液送去細菌/真菌培養、隱球菌抗原、必要時結核菌PCR;從血清中檢查CMV PCR;眼科散瞳檢查
皮膚
- 嗜酸性毛囊炎;疣(HPV);HSV及VZV;MRSA軟組織感染;疥瘡;念珠菌感染;濕疹;結節性瘙癢症;牛皮癬;藥物皮疹;指甲下真菌病
- 軟疣(poxvirus):2-5 mm 的珍珠狀丘疹,中央有凹陷
- 卡波西氏肉瘤(KSHV或HHV8):紅紫色非褪色結節性病變
- 桿菌血管瘤(播散性Bartonella):脆弱的紫藍色血管丘疹
口腔
- 鵝口瘡;KS;口腔念珠菌病(凝乳狀斑塊,通常無痛)
- 口腔毛狀白斑:無痛的乳頭狀增生,附有白色塗層,通常在舌頭側面,由EBV引起,但不是癌前病變
眼科
- CMV視網膜炎(CD4通常<50);治療:ganciclovir或valganciclovir、foscarnet或cidofovir
- HZV、VZV、梅毒(任何CD4計數,視為神經梅毒)或弓形蟲感染(CD4通常<100)
內分泌/代謝
- 性腺功能減退;腎上腺功能不足(CMV、MAC、TB、HIV或藥物相關);肌肉萎縮;骨質疏鬆/脆性骨折(所有CD4計數)
- 脂肪重分佈症:中央肥胖、外周脂肪萎縮、血脂異常、高血糖
心血管 (JACC 2013;61:511)
- 冠狀動脈疾病、中風、靜脈血栓栓塞、擴張性心肌病;肺動脈高壓;心包炎/心包積液
呼吸系統
| 影像學模式 | 常見原因 |
|---|---|
| 正常 | 早期 PCP |
| 擴散性間質浸潤 | PCP、TB、病毒感染,或播散性真菌感染 |
| 焦點性實變或腫塊 | 細菌或真菌感染、TB、KS |
| 空洞性病變 | TB、NTM、麴菌感染、其他真菌感染、細菌感染(包括_Staph aureus_、Nocardia、Rhodococcus) |
| 胸腔積液 | TB、細菌或真菌感染、KS、淋巴瘤 |
Pneumocystis jiroveci (PCP) 肺囊蟲肺炎 (NEJM 1990;323:1444)
- CD4 <200
- 發燒、夜間盜汗、運動後呼吸困難、乾咳
- 胸部 X 光顯示間質模式,PaO2 下降,A-a梯度上升,LDH 上升,痰液 PCP 染色陽性,β-glucan 陽性
- 如果 PaO2 >70:TMP-SMX 15-20 mg/kg,分三次口服
- 如果 PaO2 <70 或 A-a梯度 >35:在抗生素治療之前使用 prednisone(40 mg 口服兩次,5 天後減少)
HIV ⊕ 吸煙者更可能死於肺癌而非伺機性感染 (JAMA 2017;177:1613)
胃腸及肝膽系統
- 食道炎:念珠菌、CMV(單一、大蛇行)、HSV(多發、小而淺)、巨大鵝口瘡、藥物引起;如果沒有念珠菌感染或對經驗性抗真菌治療無反應則安排胃鏡
- 腸炎:細菌性(尤其是急性:志賀氏菌、沙門氏菌、困難梭狀桿菌 );原蟲性(尤其是慢性:Giardia、Isospora、Cryptosporidium、Cyclospora、Microsporidium、Entamoeba);病毒性(CMV、腺病毒);真菌性(Histoplasmosis);MAC;AIDS 腸病;TB 腸炎
- 腸胃道出血:CMV、卡波西氏肉瘤、淋巴瘤、Histoplasmosis;直腸炎:HSV、CMV、LGV、淋病
- 肝炎:HBV、HCV、CMV、MAC、TB、Histoplasmosis、藥物誘發
- AIDS膽管病:通常與 CMV 或 Cryptosporidium 或 Microsporidium(CD4 下降時)相關
腎臟
- HIV 相關腎病(塌陷性 FSGS);腎毒性藥物(如 TDF → 近曲小管功能障礙)
血液學/腫瘤學 (NEJM 2018;378:1029)
- 血液學異常:ACD、腫瘤/感染(如 MAC/TB)對骨髓的浸潤、藥物毒性、溶血、免疫性血小板減少症
- 非何杰金淋巴瘤:任何 CD4 計數頻率增加,但隨著 CD4 減少而增加
- 何杰金淋巴瘤(任何 CD4;ART 的影響尚不明確)
- 中樞神經系統淋巴瘤: CD4 計數 <50,與 EBV 相關
- 卡波西氏肉瘤KS(HHV-8): 在任何 CD4 計數下,發病率因 CD4 減少而增加,通常為男男性行為者(MSM);黏膜皮膚(紫色病變);肺部(結節、浸潤、淋巴結擴大);胃腸道(出血、阻塞)
- 子宮頸/肛門癌(HPV 高風險,特別是在 MSM 中)
- 肝癌(與 HBV/HCV 相關)、胃癌
神經學/心理學
- 腦膜炎:隱球菌(使用腦脊髓液診斷;血清抗原敏感度 90%)、細菌性(包括李斯特菌)、病毒性(HSV、CMV、原發 HIV)、TB、Histoplasmosis、Coccidioidomycosis、淋巴瘤;神經梅毒(顱神經麻痺)
- 占位性病變:可能表現為頭痛、局部神經學缺損或意識改變。檢查:MRI,腦部切片僅在懷疑非弓形蟲病病因(弓形蟲血清學陰性)或對2週經驗性抗弓形蟲治療無反應時進行(弓形蟲感染50% 於第 3 天治療有反應,91% 於第 14 天;NEJM 1993;329:995)
| 病因 | 影像學表現 | 診斷研究 |
|---|---|---|
| 弓形蟲感染 | 增強病變,通常在基底神經節(可以是多發性) | ⊕ 弓形蟲血清學(敏感度約 85%) |
| 中樞神經系統淋巴瘤 | 增強環狀病變(單發性 60%) | ⊕ CSF PCR 檢查 EBV ⊕ SPECT 或 PET 掃描 |
| 進行性多灶性白質腦病(PML) | 白質中多發性非增強病變 | ⊕ CSF PCR 檢查 JC 病毒 |
| 其他:膿瘍、分枝桿菌感染、隱球菌感染、TB、CMV、HIV | 不一定 | 切片 |
- HIV 相關癡呆症:抑鬱症狀、注意力/集中力受損、精神運動遲緩
- 抑鬱症:自殺/抑鬱症發病率增加
- 脊髓病變:感染(CMV、HSV)、脊髓壓迫(硬膜外膿瘍、淋巴瘤)
- 周邊神經病變:藥物(尤其是第一代NRTIs)、CMV、糖尿病
全身性鳥型分枝桿菌感染(DMAC)
- 發燒、夜間盜汗、體重減輕、腹痛、腹瀉、全血球減少。可引起局部淋巴結炎
- 治療:clarithro/azithro + ethambutol ± rifampin/rifabutin
巨細胞病毒(CMV)
- 視網膜炎、食道炎、結腸炎、肝炎、神經病變、腦炎
- CMV 病毒量可能為陰性
- 考慮組織切片
- 治療:ganciclovir、valganciclovir、foscarnet 或 cidofovir
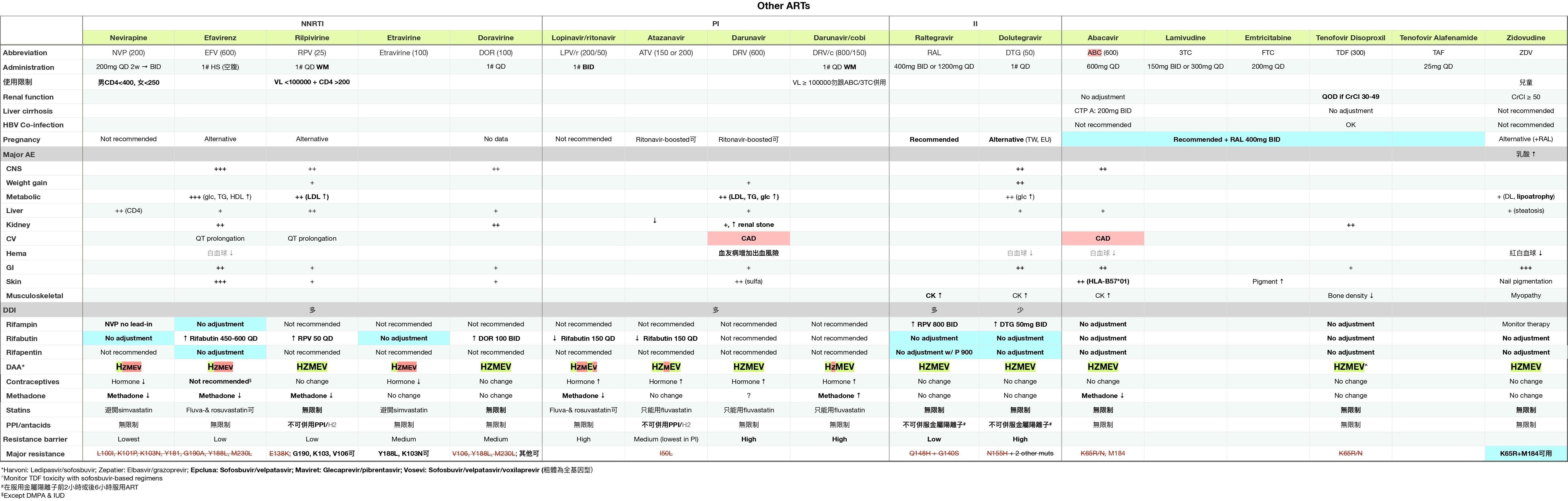
抗病毒藥物
考古題
專師
// Specify the path to the original note
const originalNotePath = "Area/Medicine/專師考試解題.md"; // Replace with your actual file path
// Read the content of the original file asynchronously
const content = await app.vault.read(app.vault.getAbstractFileByPath(originalNotePath));
// Define the tag you're searching for
const tag = "#medicine/HIV"; // Replace with your actual tag
// Split the content into sections based on the start of a new question (line with a number and a period)
const sections = content.split(/(?=\d+\.\s)/);
// Initialize an array to store the results
const results = [];
// Process each section
sections.forEach(section => {
if (section.includes(tag)) {
// Add the section to results if it contains the tag
results.push(section.trim());
}
});
// Output the captured sections
results.forEach(result => dv.paragraph(result));
內科醫師
// Specify the path to the original note
const originalNotePath = "Area/Medicine/內專考古題.md"; // Replace with your actual file path
// Read the content of the original file asynchronously
const content = await app.vault.read(app.vault.getAbstractFileByPath(originalNotePath));
// Define the tag you're searching for
const tag = "#medicine/HIV"; // Replace with your actual tag
// Split the content into sections based on the start of a new question (line with a number and a period)
const sections = content.split(/(?=\d+\.\s)/);
// Initialize an array to store the results
const results = [];
// Process each section
sections.forEach(section => {
if (section.includes(tag)) {
// Add the section to results if it contains the tag
results.push(section.trim());
}
});
// Output the captured sections
results.forEach(result => dv.paragraph(result));